
The cardio-thoracic sphere
By simplifying
Thoraco-diaphragmatic mechanics
The thoraco-diaphragmatic cage functions like an accordion placed vertically.
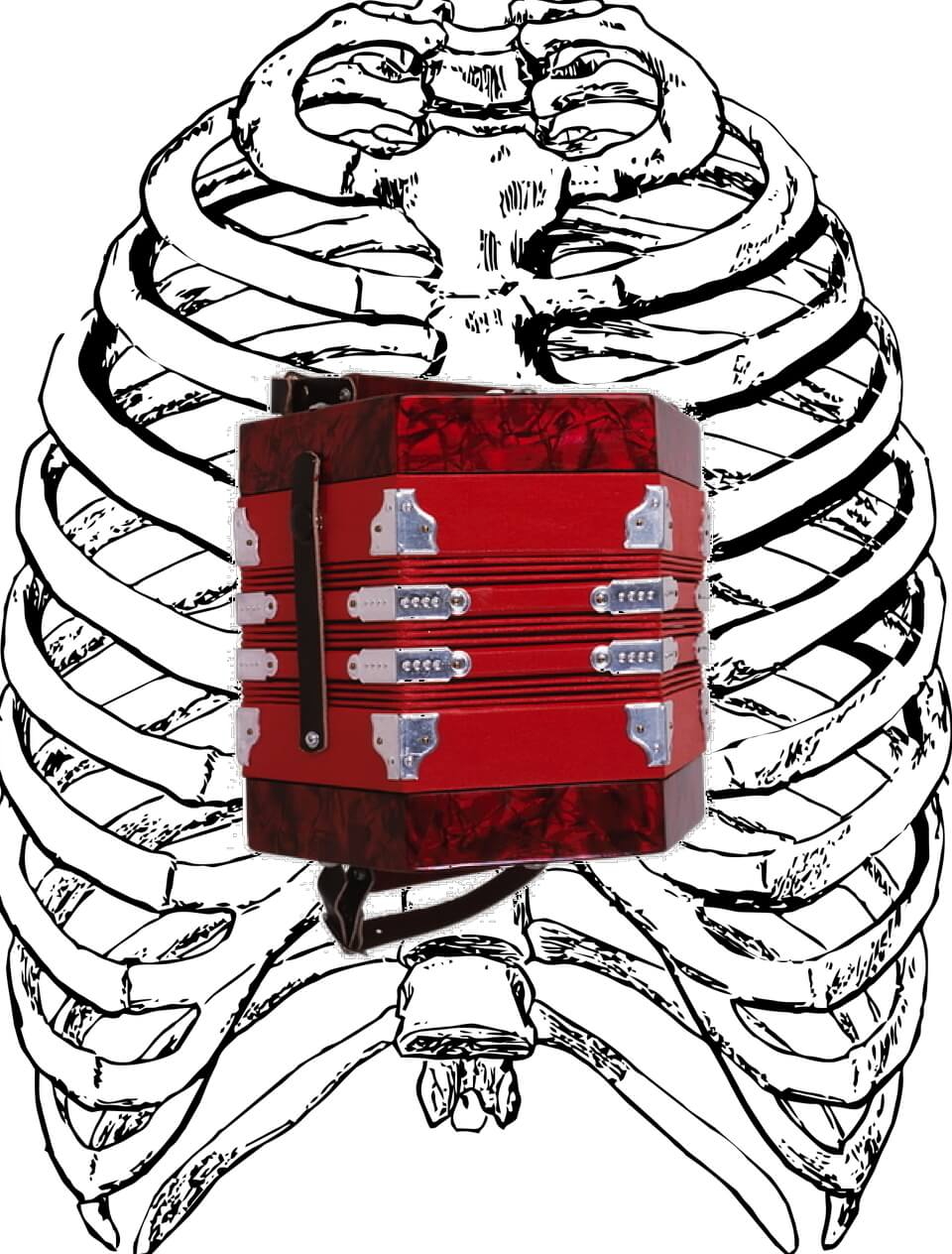
When you breathe the upper ribs raise one end of the bandoneon while the lower ribs and diaphragm will lower the other end .
The upper part (the upper ribs) will rise while the lower part (the lower ribs and the diaphragm) will fall during inspiration.
The ribs will all move away from each other during this inspiration, thus increasing the volume of the rib cage.
However…
We don’t necessarily breathe evenly. We can breathe:
- Only with the upper chest
- Only with the lower part (lower chest and diaphragm)
- With the two modes above
- Or the diaphragm can work alone (without the ribs, neither lower nor upper)
The breathing mode will depend on our activity, there is no good or bad breathing, there are simply breathing modes adapted to the effort or not.
To become aware of these two types of breathing you can put your hands on your lower ribs laterally and slightly backwards :
“Breathe in with your upper chest and you will feel your ribs rise”;
“Breathe in with your belly and lower chest and you will feel your ribs slide down and forward…”
“Breathe in just with your stomach, you’ll feel your ribs sliding down and forward much less, the contraction of the diaphragm and an abdominal oblique intervening in the mobilization of the ribs downwards (so without raising them)…”
Of course we will have lesional breathing patterns (intercostal spasms preventing the ribs from unfolding, diaphragmatic atony, etc).
It is logical that the lower ribs drive the diaphragm downwards during diaphragmatic inspiration, in fact 1cm of lowering of the torque (lower ribs and diaphragm) increases the volume of the lungs by 500cm3.
Lesions of non-acquisition:
Some patients do not know how to breathe with the upper part of the thorax, others have no control of their diaphragmatic breathing. Rarely both at the same time, or only partially…
The treatment will be to make the patient aware of this deficiency and to teach him/her to breathe with the upper or lower part of the rib cage .
Lesions of muscle and/or joint spasms:
Respiratory mechanics and good ventilation depends on the good quality of all the joints of the body and the tonic balance of all the muscles of the body. For example, a lesion in the anterior rectus muscle of the thigh leading to a lesion of the 12th rib will be detrimental to diaphragmatic breathing… A lesion in one of the wrist bones will act on one of the first 7 ribs…
Each joint and/or muscle injury will have an impact on the subject’s ventilation. A globalist vision of the subject is a reality…
Lesions of the intercostal muscles:
Although they are only minimally involved in the ventilation of the upper costal grill (first 7 ribs), they could be of decisive importance for the lower ribs in terms of the downward displacement of diaphragmatic amplification, even minimally.
If the intercostal muscles are “spasmed”, the ribs between which they are found will move closer together. This will cause a decrease in the volume of air in the lungs. To compensate for this loss of volume in the upper part, the diaphragm will increase its tension and lower itself to increase the volume of the lower part. The stroke of the diaphragm’s inspiratory and expiratory work will be almost the same or even slightly reduced, but the diaphragm will be lowered by increasing its tone…
Stress represents this type of lesion, which forms the backdrop for many symptoms and even pathologies.
Costal lesions will lead to a lowering and an increase in diaphragmatic tension. And the greater the tension of the intercostals, the greater the tension of the diaphragm. Consequently, the abdominal tension will increase, which will require an overload of work on the diaphragm. The vicious circle is set in motion…
Consequently, any costal injury will have an impact on the diaphragm, which will suffer from it. Releasing the diaphragm without first releasing the costal grill will not give the best results.
Pre-delivery treatments using “Ad Hoc” treatment of the rib grill gives a 30% higher FEV6 (Maximum Expiratory Ventilation for 6 seconds) than other osteopathic treatments of the diaphragm.
Hemodynamic Osteopathy takes against the current theories concerning all respiratory insufficiencies. We classify them as pathologies of inspiratory insufficiencies and not the opposite. Translated with www.DeepL.com/Translator (free version)
The different types of breathing patterns and lesions:
In the first place inspiration is defined by the distance between the ribs.
A “normal” breath should see the upper ribs rise and the lower ribs and the diaphragm descend.
But both types of breathing adapt to your activity.
If you work with your upper limbs you will tend to breathe with your stomach.
If you work with the lower limbs you will tend to breathe with the upper ribs.
But when breathing the ribs can be raised by raising the sternum (among other things).
We can breathe with a permanently raised sternum or on the contrary with a sternum that never rises and remains in a low position .
Add to this lack of amplification the fact that the intercostal muscles can be “spasmed” and you will find yourself facing different phenomena of thoracic deformities…
But it’s not all that simple…
Indeed the rib cage develops in three dimensions.
From top to bottom as we saw above…
Laterally the ribs will move apart on inspiration.
From front to back, when breathing in, the upper part of the sternum will move forward more than the lower part of the sternum.
We will then be able to find phenomena of :
- Cyphosis (classic)
The ribs will be brought closer together by the contraction of the intercostal muscles.
The muscles are located between the ribs, so their contraction is (among other things) to bring them closer together.
The exhalation of the thorax will cause the spine to function in expiration and thus in kyphosis.
It is useless to try to treat a cyphosis without first treating the cause, i.e. the thoracic closure…
Once the thoracic opening has been obtained, straightening the spine becomes easier and some exercises can accelerate the return to a more erect posture.
Of course, a kyphosis fixed by the years will be much more difficult to treat than that of a pre-adolescent…
Xiphoid funnel

The ribs will be brought closer together by the contraction of the intercostal muscles.
The muscles are located between the ribs, so their contraction is (among other things) to bring them closer together.
The exhalation of the thorax will cause the spine to function in expiration and thus in kyphosis.
It is useless to try to treat a cyphosis without first treating the cause, i.e. the thoracic closure…
Once the thoracic opening has been obtained, straightening the spine becomes easier and some exercises can accelerate the return to a more erect posture.
Of course, a kyphosis fixed by the years will be much more difficult to treat than that of a pre-adolescent…
- Xiphoid funnel

In this case the lower part of the sternum is in front of the upper part. It is important to treat these children as early as possible…
- From thorax to barrel
It is also a lesion of the costal grill in expiration… But this time in elevation (of the upper ribs with the sternum) this one is raised permanently, the patient desperately tries to breathe in. He breathes only with the diaphragm. The treatment will be to open the chest (freeing the intercostals), lower the sternum and teach him to breathe with his rib cage.
- Sigaud’s Fins
We can also have diaphragmatic breathing with low ribs spasmed in inspiration (they remain positioned forward and down).
Concerning the diaphragm
There was no mention of any diaphragmatic work in the above treatments.
Of course we have to remove the diaphragmatic lesions, but the results of the costal grid treatments are much better than the diaphragm treatments.
The diaphragm just needs to function freely, free all parasitic lesions and stress and it will return to normal physiology in most cases .
Concerning the intercostal muscles, there are three types with different mechanical physiologies. They are mainly involved in maintaining the costal grill when it must serve as a support point during the efforts of the upper limbs. Their active intervention during breathing is questionable since their action is to bring the ribs closer together, which would be completely counterproductive . And the ribs move apart during inspiration. Of course they can intervene during forced exhalation, simple exhalation is relatively passive. But spasms of these muscles will intervene strongly during breathing but as lesional agents…
The heart square is in the center.
The pericardium.
It is attached by the superior ligaments of the pericardium which are inserted on the last cervical vertebrae, the first dorsal and the posterior face of the sternum.
It is inserted at the bottom of the diaphragm.
Virtually every structure in the body needs movement to drain it…
Imagine the heart hanging between the cervical vertebrae and sternum at the top and the diaphragm at the bottom.
Tension of the intercostal muscles will automatically cause the diaphragm to descend. The pericardial tissues and their contents will be stretched, permanently taut. The pericardial tissues and their contents will be stretched and stretched permanently. The pericardial system will be weakened by insufficient drainage, congestion and lack of vascularisation…
Lack of physiological drainage, congestion, lack of tissue vascularization are the open door to inflammations and infections of all kinds…